Compliance automations that protect you against penalties.
Enjoy peace of mind knowing Practice Pro compliance technology helps you stay ahead of ever-increasing and changing regulations for physical, occupational, speech, and pediatric therapy practices.
.
Rules in Check
Compliance is built-in and automated throughout the different workflows within the EMR system – from scheduling to documentation to billing.
Peace of Mind
With safeguards in place, Practice Pro’s web-based EMR is a trusted solution where rules integrate, and your data is always protected.
Automations
Automation is the key to delivering effective and compliant care. Our robust rule engines automatically enforce payer-specific rules, leaving your providers to focus on what matters the most – better care.
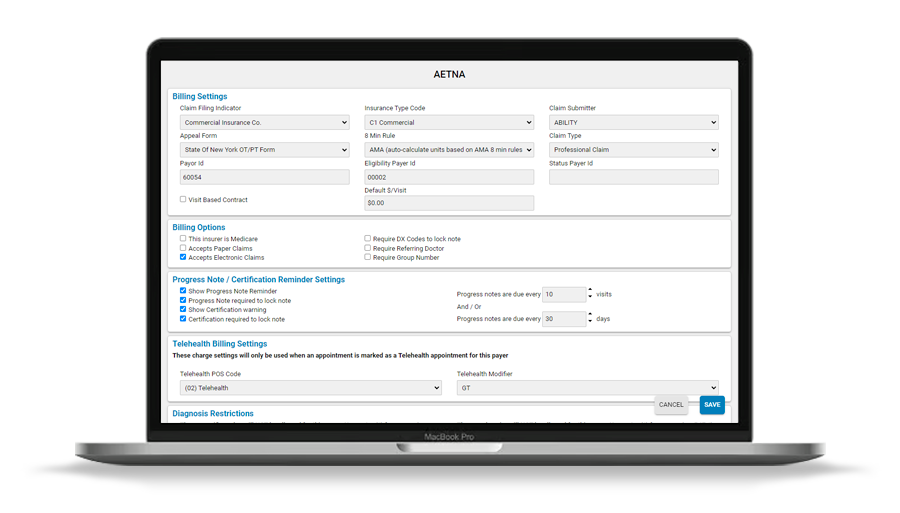
Medicare 8-Minute Rule:Accurate physical therapy billing requires integrated intelligence to comply with the Medicare 8-minute rule for time-based codes; that’s why Practice Pro automatically manages timed and untimed code differentiation.
Therapy Cap: Tracking, alerts, and our automatic KX modifier application help to prevent loss of payment.
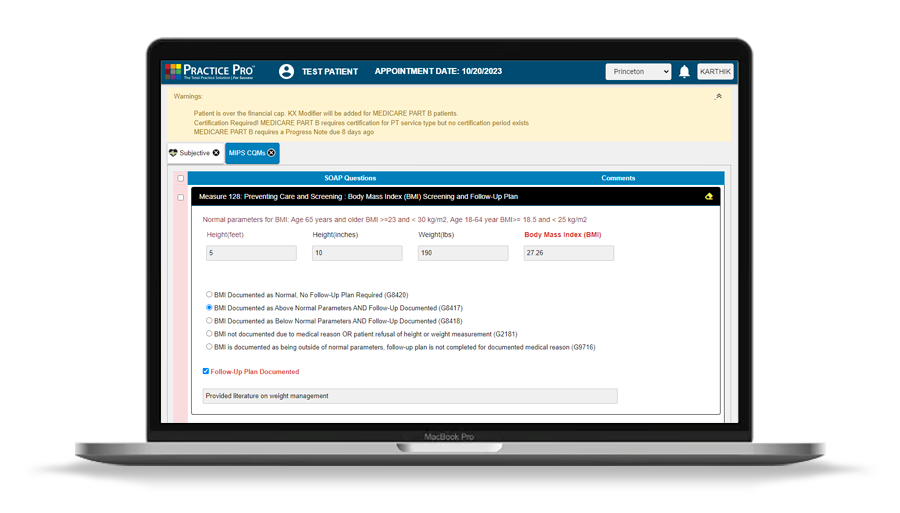
MIPS: A therapist’s MIPS performance score is based on two weighted categories: quality measures and improvement activities. Because Practice Pro is a qualified MIPS registry, we make MIPS reporting a breeze.
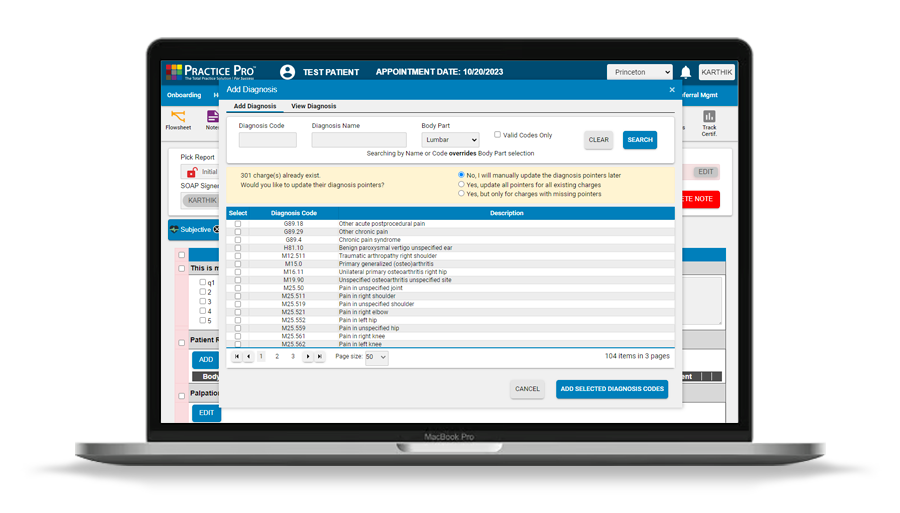
ICD-10 Codes: ICD-10 coding, designed to enable therapists to provide more accurate documentation required for reimbursement, is a seamless and automated process with our all-in-one solution. The proper codes are continuously captured and transmitted to billing to ensure on-time payments.
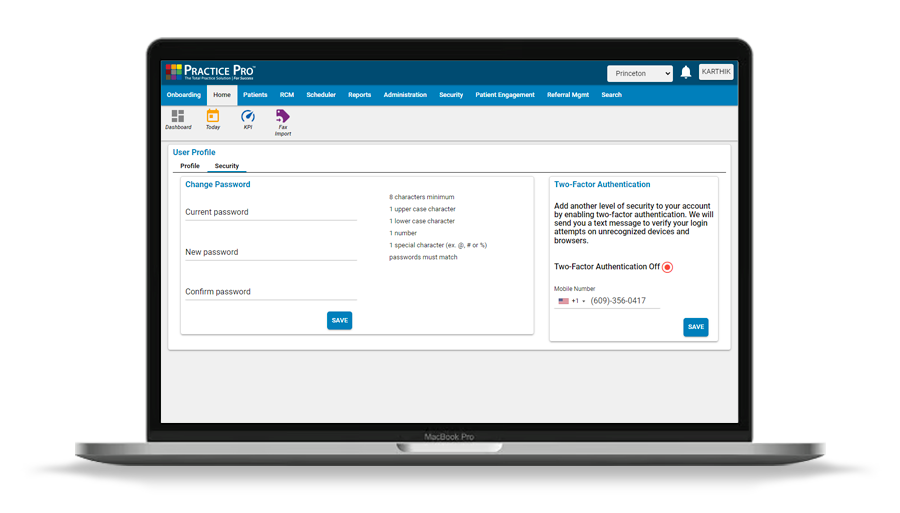
HIPAA governs how physical therapists and other providers handle protected health information (PHI). A single breach could expose a practice to steep fines. With the use of iron-clad security and top tier data centers we ensure that PHI is safe and protected.